The Rehabilitation Program European Theater of Operations APO # 871
Group picture illustrating ETO Chief Surgeon’s staff, at Cheltenham, England, November 1942. Brigadier General Paul R. Hawley, Chief Surgeon (1) Colonel Eli B. Brown, Chief Hospitalization Division (2) Colonel William S. Middleton, Chief Consultant Medicine (3) Colonel James B. Mason, Chief Operations Division (4) Lieutenant Colonel John E. Gordon, Chief Preventive Medicine Division (5) Captain Margaret E. Aaron, Chief Nursing Division (6) …
Introduction:
The overall scope of the Program was to hasten the return of patients to active duty. The mission of the Medical Department was “the conservation of manpower – the preservation of the fighting strength of the military forces”.
Rehabilitation activities in the Office of the Chief Surgeon had already begun on the initiative of Lt. Colonel Rex L. Diveley, MC (Senior Consultant Orthopedic Surgery –ed).
Each convalescent patient was graded periodically by his Medical Officer. His activities were prescribed in accordance with his rate of recovery and his MOS. The overall program was adapted to Theater requirements and proportioned among physical and military reconditioning and recreational diversion.
The program was a success because it furnished those disabled patients with such hospitalization facilities as would speedily restore them to good health and fighting efficiency. It was not sufficient to cure the patient of his disease or injury; it was necessary that the proper treatment cover the entire period until he was physically and mentally fit to return to his unit. The Rehabilitation Program effectively covered that phase, from the time the soldier became a convalescent patient and could leave the hospital until he had completely recovered and could return to his unit!
Training in Rehabilitation Exercises:
The Chief Surgeon ETOUSA, Brigadier General Paul R. Hawley, MC, directed with Circular Letter C/S No. 146, dated 27 September 1943, Subject: “Rehabilitation Program” that a physical rehabilitation and educational program be started in all Hospitals (in the United Kingdom –ed) without delay. A review of the major training in Rehabilitation Exercises was distributed to all Base Section Surgeons and Commanding Officers of Station and General Hospitals located in the United Kingdom Base (at the beginning of 1943, General P. R. Hawley’s office contained 11 different Divisions; Administration – Hospitalization – Supply – Personnel – Preventive Medicine – Professional Services – Operations & Training – Medical Records – Nursing – Dental and Veterinary, they were eventually multiplied, combined, and reorganized during the following years; his staff included 51 Officers – 56 Enlisted Men and 62 civilians –ed).
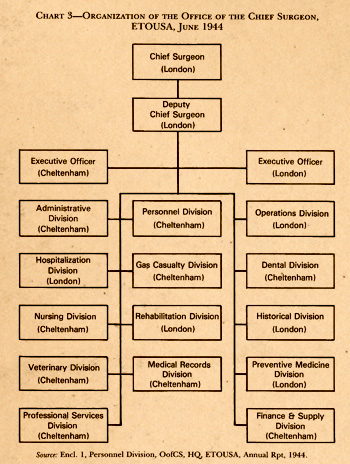
Chart illustrating the early June 1944 organization of the Office of the Chief Surgeon, ETOUSA in the United Kingdom.
The CO, 8th Convalescent Hospital, had recently discussed this program with all interested parties and indicated a series of exercises for muscle re-education. Physical rehabilitation, to a large extent, was to be conducted by Medical Department Enlisted personnel at each hospital under the direction of a specially trained Non-Commissioned Officer.
A two-weeks instruction course was to be instituted at the 8th Convalescent Hospital, Stoneleigh, Warwickshire, for the training of the NCOs from the Station and General Hospitals. A total of eight (8) Non-Commissioned Officers was to be trained at each course, and courses were to be continued until one (1) NCO from each Hospital had been trained! Commanding Officers were instructed to make a careful selection of the NCO to conduct the program and give special attention to the development of a cogent program.
The selected Non-Commissioned Officer was instructed to train sufficient Enlisted Ward Attendants to insure that Rehabilitation exercises be conducted on each Hospital Ward. Trained War Attendants, in turn, were supposed to instruct selected ambulatory patients in conducting these exercises.
The initial course for NCO instruction was to start 18 October 1943. Each Hospital Commander was therefore instructed to submit to his Base Section Surgeon, the name – rank – and serial number of the NCO designated to attend. Orders were to be published and distributed by the respective Base Sections.
Convalescent Rehabilitation in Hospitals:
On behalf of the Chief Surgeon, Colonel Charles B. Spruit, MC, Deputy Chief Surgeon ETOUSA, distributed Circular Letter C/S No. 168, dated 8 November 1943, explaining the basics for the Convalescent Rehabilitation of Patients treated at Hospitals in the United Kingdom.
The general purpose of the Rehabilitation Program was the return to duty of service personnel, recovering from disease or injury, in the best possible physical and mental condition through the use of planned physical conditioning and the constructive use of leisure time in educational pursuits designed to effect a greater realization of personal importance and produce a more informed soldier.
It wasn’t enough for the Medical Officer to aid and promote healing. There was also the need to restore physical health and vigor and to foster the mental toughness so essential for effective military duty. The Officer was expected to create the desire to get well and the expectancy of further service.
Hospitals that had already carried out intensive Rehabilitation programs found out that:
- men were returned physically fit for full duty
- re-admissions to the hospital were effectively reduced
- the period of convalescence was shortened in certain cases of acute infectious and contagious diseases
- morale and fighting spirit were improved
The Rehabilitation Program included four (4) different classes of patients (called “trainees” by the local staff –ed) for ease of administrative handling.

Pictures illustrating aspects of general rehabilitation activities, military training, and occupational therapy conducted at the Convalescent Centers.
Class “A” > comprised that group nearest to the point of recovery – daily physical training was to enable them to engage in an eight-hour activities program that would allow them to pass a physical fitness test and carry out a twelve-mile hike before return to duty.
Class “B” > included those ambulatory patients capable of six hours of physical training, comprising calisthenics, drill, marches, outdoor fatigue, and athletics.
Class “C” > were ambulatory hospital patients still receiving treatment which was paramount but who were only confined to bed a portion of each day. They were divided into groups for medically supervised exercises according to anatomical limitations such as upper and lower extremity, abdominal, and special cases. Frequent rest periods were essential.
Class “D” > consisted of patients considered convalescent but still bed cases or confined to the medical ward.
Note: The basic program for Class “C” and “D” were high in educational pursuits but low in physical training. As convalescence progressed; it became higher in physical training and proportionately lower in educational subjects. This program was designed to produce gradual progress and improvement in strength and resistance to the point where the patient could be discharged from the hospital and assume full military duty without physical injury to himself.
It was important to begin Rehabilitation while the patients were still in the hospital ward. It was equally underlined to introduce the Rehabilitation Program as soon as the convalescence was begun.
The success of convalescent training (patients were designated “trainees” –ed) was based upon adequate medical supervision of the convalescent’s activities. The patient’s pride assisted him in mastering the initial phases. As convalescence progressed, the soldier was able to consult his physician and follow his advice. Experience showed that when the Convalescent/Rehabilitation/Reconditioning Programs were properly conducted, the patient/trainee enjoyed the process of getting well. It was important for morale that wholehearted effort and optimistic enthusiasm be directed by hospital personnel toward the success of this Program.
Physical Training:
The physical training during the hospital ward phase consisted of the following:
- physical therapy
- heliotherapy
- medically supervised exercise, such as rolling, stretching, light arm and foot movements, consistent with limitations imposed by disease or injury
- limited exercise under supervision, outdoors but adjacent to the wards
- recreational equipment to be provided for ping pong, table games, playing catch, horseshoes, etc., with the American Red Cross supplying materials for this purpose
- ward fatigue
- occupational therapy

Major Frank E. Stinchfield, during a demonstration held for student Officers at the Rehabilitation Center No. 1, Bromsgrove, England, in July 1943.
Rehabilitation Training:
The Chief Surgeon, ETOUSA, as part of the general Hospital Rehabilitation Program in operation, instituted and conducted a program of military training based on the physical capability of the patients. Its purpose was to vary with the type of hospital and the stage of convalescence, and was in no way to curtail or restrict the active medical and surgical care of the patients/trainees.
The program for patients in the early phase of Rehabilitation emphasized individual training in Physical Conditioning and Basic Military Training.
The program for patients in the later phase of Rehabilitation emphasized team work and unit/group training in Physical Conditioning, Basic Military Training, and Technical Military Training.
Educational Program:
Interesting, helpful, informative, and educational talks and discussions were to be brought to the bedside in the wards. Later, a central point could serve for lectures and demonstrations. About two hours daily were to be reserved for classes in military instruction, training films, and in general education.
Administration:
Personnel > The Hospital COs were to appoint a Rehabilitation Officer to organize, plan, and supervise the program. The Medical Department Officer chosen for this work was to be capable of enthusiastic and dynamic direction.
Officer patients were to be freely used to supervise reconditioning and Enlisted Men from the patient group, having had combat experience and/or special abilities, were to be utilized in the overall training program.
General Hospitals caring for patients returned from combat found it desirable to employ in the Rehabilitation Program, Officers and EM who had had previous combat experience overseas or long service with tactical units. Common experiences shared enabled the patient to “understand the language” of the instructor.
It was recommended to make use of the Chaplain, the American Red Cross staff, the Instructors on the post, air base, camp, or station. Guests speakers were to be invited from the community and from adjacent educational and cultural institutions.
Policies for Admission > Training was to start at the earliest possible time after convalescence was begun. It was highly recommended to combat idleness and boredom in the hospital with interesting directed activity.
It was underlined that any patients capable of a prompt return to full duty after a short illness were NOT to be retained in the hospital for the rehabilitation training.
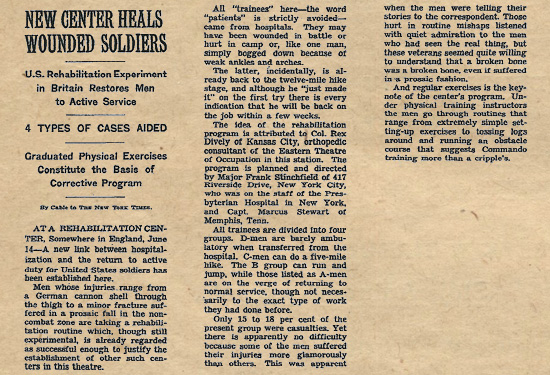
Article published in the New York Times, dated 15 June 1943, describing the introduction of the US Army Rehabilitation Program being experimented in the United Kingdom (Courtesy Isabel Cymerman).
The Rehabilitation activities to be conducted by General and Station Hospitals were not meant to replace the need for or the use of rehabilitation activities in Convalescent Hospitals (as per instructions dated 19 Oct 43, selected patients who could not be returned to duty within fourteen (14) days were to be transferred to the 8th Conv Hosp – those patients who could return to duty within fourteen (14) days were logical candidates for General and Station Hospital Rehabilitation Programs –ed).
It was important to maintain medical supervision at all times over all aspects of the training program to prevent any harmful overdoing and to encourage advancement. It was recommended that once a week a representative specialist in the field of the original disability examine the patient to insure satisfactory progress.
The Medical Officer in charge of the Rehabilitation Program was to accept responsibility for the indoctrination of all other Medical Officers, Nurses, and other personnel in the General or Station Hospital, in the principles of rehabilitation for duty.
Records > A questionnaire proved helpful to discover instructor material and interests among the different patient groups.
The dearth of scientific medical information concerning convalescence gave an unparalleled opportunity for accumulation of valuable data and findings for future use to medicine.
Equipment and Funds > The purchase of special athletic and recreational equipment for use of patients in the Rehabilitation Program was deemed a proper expenditure from the Hospital Fund, when not obtainable through the Base Section Special Service Officer.
Educational, Recreational and Training Aids available in the European Theater of Operations:
Procurable through Base Section Special Service Officer > These included recreational, athletic, educational, and musical equipment. Also foreign language kits (French, German, Italian) were considered, accompanied with linguaphone language classes. Correspondence study, under the auspices of the US Armed Forces Institute was also provided. Motion picture projector equipment and pamphlets, general interest books and magazines, and special and/or technical books could be procured.
Procurable through Base Section Training and Security Officer > Aircraft models for proper identification could be made available.
Procurable through Base Section Signal Officer > With the assistance of the Army Pictorial Service, training films, film bulletins, combat bulletins, and film strips were provided. Also included were orientation films, Army-Navy movies, and GI movies.
Procurable through Adjutant General’s Office, Services of Supply > Charts, graphic training aids, and miscellaneous posters.
Procurable through Base Section Adjutant General’s Office > Technical Manuals, Field Manuals, and miscellaneous Technical Bulletins.
Suggested Rehabilitation Program in a Hospital Ward, General or Station Hospital:
| Time | Duty |
| 0800 – 0900 | Ward fatigue, ward rounds |
| 0900 – 1000 | Lecture |
| 1000 – 1100 | Calisthenics, physical therapy, occupational therapy |
| 1100 – 1200 | Dinner |
| 1200 – 1300 | Rest |
| 1300 – 1400 | Reading, book review, educational course, study |
| 1400 – 1500 | Hobby hour, occupational therapy, ARC arts & crafts |
| 1500 – 1600 | Lecture |
| 1600 – 1700 | Supper |
| 1800 – 2100 | Recreation (ward games, group singing, musical entertainment, etc.) |
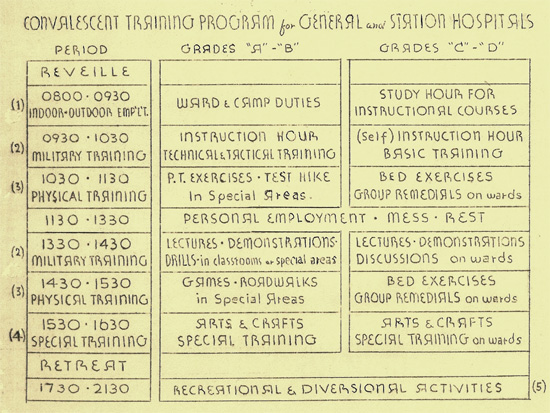
Chart illustrating the different Convalescent Training Programs in use at General and Station Hospitals in the United Kingdom.
Official Organization:
On 25 February 1944, Colonel Rex L. Diveley was appointed Director of Rehabilitation (to supervise all Convalescent Rehabilitation Centers) in addition to his other duties as Senior Consultant in Orthopedic Surgery. His assistant was Major Marcus J. Stewart, MC. As Rehabilitation work increased, more Officers and administrative personnel joined the Rehabilitation Division staff.
Transfer of Patients to Convalescent Facilities:
With Administrative Memorandum # 63, File 704.11, dated 12 May 1944, the Surgeons at the different Base Sections as well as the Commanding Officers of all General and Station Hospitals were duly informed that the following Convalescent facilities were established in the United Kingdom:
Reconditioning Center No. 1 > Erlestoke Park, with railhead at Devizes, Wiltshire – 77th Station Hospital
Rehabilitation Center No. 1 > Stoneleigh Park, with railhead at Leamington Spa, Warwickshire – 307th Station Hospital
Rehabilitation Center No. 2 > Bromsgrove, with railhead at Bromsgrove, Worcestershire – Detachment B, 77th Station Hospital (later taken over by 123d Station Hospital –ed)
Neuro-Psychiatric Rehabilitation Center > Shugborough Park, with railhead at Stafford, Staffordshire – 312th Station Hospital
Note: With the increasing patient census following operations on the Continent, an additional number of rehabilitation beds became necessary. New units were selected and after proper indoctrination, conversion and training two additional centers were established:
Rehabilitation Center No. 3 > Fremington, Devonshire (later Warminster Barracks, Wiltshire) – 313th Station Hospital
Rehabilitation Center No. 4 > Honiton-Heathfield, Devonshire – 314th Station Hospital
When no remedial exercises or treatment were needed, the convalescent patient (except Army Air Force personnel) was to be sent to a Reconditioning Center where general physical exercises were given to restore him to his former physical capacity. All Enlisted Men (except Army Air Force) requiring reconditioning were to be transferred to Reconditioning Center No. 1. All Officers requiring reconditioning were to be sent to Rehabilitation Center No. 2. All Enlisted Men, Army Air Force, requiring reconditioning were to be transferred to Rehabilitation Center No. 1. It should be noted that cooperation of the Army Air Forces was rather meager at the beginning, but liaison was maintained and specialized personnel eventually obtained (as a matter of fact, Flight Surgeons were selected and went to duty with the 6 General Hospitals caring for AAF personnel –ed). Special surveys were made to determine the needs of the Rehabilitation Program destined for the US Army Air Forces and training aids and equipment supplied to all General and Station Hospitals and Convalescent Centers.
Information Letter Number Ten, dated February 1944, ref. 4-6276, AF (first page) covering the Army Air Forces Convalescent – Rehabilitation Training Program describing its working methods and how to obtain the best results with the program (Courtesy Pieter Dejonghe).
When special remedial exercises were needed to restore a particular part of its normal function, the convalescent patient was to be sent to a Rehabilitation Center. Such patient included most of the orthopedic and extremity cases, herniotomies, and all other cases requiring remedial exercises or treatment.
All Enlisted Men requiring the above were sent to Rehabilitation Center No. 1. All Officers requiring rehabilitation were transferred to Rehabilitation Center No. 2.
When N-P rehabilitation was required, the convalescent patient was to be sent to the Neuro-Psychiatric Rehabilitation Center.
Note: The Hospital CO desiring to transfer patients for either Rehabilitation or Reconditioning was to contact the Commanding Officer of the proper Camp or Center to determine the availability of accommodations.
Further Organization:
With Letter C/S and Office of the Chief Surgeon, Order No. 32, dated 3 June 1944, the Rehabilitation Division was formerly established as an independent division. Colonel Rex L. Diveley, MC, was appointed Chief of the new Division. The major functions were as follows:
- to direct and conduct research in Rehabilitation procedures
- to control Rehabilitation technical operations
- to direct the training of personnel for implementation of the Rehabilitation Program
- to formulate policies on Rehabilitation
- to consult on matters relating to conservation of manpower
With regard to the conversion of 750-bed Station Hospitals to 3,000-bed Convalescent Centers (discussed with the Office of the Chief Surgeon 28 April 1944) it was felt that medical personnel of one 750-bed Sta Hosp would be able to staff two 3,000 Convalescent Centers.
It was however concluded, that better results would be obtained by using one supplemented 750-bed Sta Hosp to activate one 6,000-bed Convalescent Center.
T/E required for a 6,000-bed Conv Cen would be twice that noted in T/E, dated 15 April 1944, 3,000-bed Rehabilitation Center.
The list of supplementary personnel to the Sta Hosp would include 70 Branch Immaterial Officers and 300 Branch Immaterial Enlisted Men.
On 16 June 1944, an important conference was held with G-1 and G-3 ETOUSA Staffs and the Field Force Replacement System to clarify and draft the obligations of the Chief Surgeon in carrying out the Rehabilitation Program in the Theater. When the forward echelon of the Office of the Chief Surgeon moved from the United Kingdom to the Continent on 12 July 1944, the Rehabilitation Division remained in the United Kingdom and was eventually attached to the Office of the Surgeon, United Kingdom Base. By the latter part of June, Base Section Surgeons had appointed Rehabilitation Officers to their staffs. Major William M. Brewer, MC, was appointed in the Western Base Section, and 1st Lieutenant Robert S. Rice, MAC, was appointed in the Southern Base Section.

Convalescent patients/trainees at the 307th Station Hospital, Stoneleigh, England, negotiate a Jacob’s Ladder on the obstacle course. Picture taken in fall of 1943.
With the steady growth of both the Rehabilitation and Reconditioning Programs, it was necessary to train additional Officers and EM for use in the activation of new centers. An initial allotment of 50 Officers and 100 Enlisted Men was made available, but as the increase of rehabilitation activities continued, the Ground Force Replacement System (formerly Field Force Replacement System –ed) was requested to provide additional personnel for training as instructors for the Convalescent Training Programs. On 6 July 1944, an additional 100 Officers and 300 EM were made available.
In August 1944 a request was made that a Rehabilitation Division be established in the Office of the Surgeon, United Kingdom Base. Major M. Brewer (promoted by Colonel R. E. Diveley to head the inspection and educational responsibilities for rehabilitation units in both the WBS and SBS –ed), who had previously been the Rehabilitation Officer for the Western Base Section, was appointed Chief of this subdivision of Rehabilitation in the Office of the Surgeon, United Kingdom Base. He selected a staff of Officers and Enlisted assistants. Several publications were issued by the Rehabilitation Division, describing essential exercises for both patients and ward masters as well as types of remedial apparatus for use by convalescent patients/trainees. Special motion pictures were prepared and distributed describing and demonstrating the Convalescent Training Program and the Physical Training Instructors’ responsibilities and activities. During August and September 1944, several conferences and meetings were organized in order to exchange ideas, methods of indoctrination, and discuss the demonstration of a ‘model convalescent training program’.
At the request of the Chief Surgeon, a decision was taken to organize an “Amputee Morale Team” in November 1944. The Team was to visit all hospitals and demonstrate the use of prostheses and show a movie about patients having lost extremities. This action greatly boosted morale of those soldiers having lost limbs.
Conversion & Evolution:
As the first Rehabilitation and Reconditioning Centers were operating it became clear that the selected T/O & E strength for a basic 750-bed Station Hospital did not provide for sufficient personnel with the appropriate qualifications to operate such a large Rehabilitation Center. Therefore new Tables of Organization and Equipment were created for 1,000-bed Reconditioning and 3,000-bed Rehabilitation Centers and forwarded to the Office of the Chief Surgeon approval. Formal approval followed and effective conversions started early December 1944 with 5 Station Hospitals being disbanded, converted, re-activated, and designated as follows:
The old 77th Station Hospital (Reconditioning Center No. 1) was re-designated 825th Convalescent Center (Packington Park, Great Packington, Warwickshire) with a 3,000-bed capacity; the old 307th Station Hospital (Rehabilitation Center No. 1) was re-designated 826th Convalescent Center (Stoneleigh Park, Kenilworth, Warwickshire) with a 3,700-bed capacity; the old 313th Station Hospital (Rehabilitation Center No. 3) was re-designated 827th Convalescent Center (Barton Stacey, Hampshire) with a 3,000-bed capacity; the 314th Station Hospital (Rehabilitation Center No. 4) was re-designated 828th Convalescent Center (Bromsgrove, Worcestershire) with a 2,300-bed capacity; and the old 123d Station Hospital (Rehabilitation Center No. 2) with limited resources was finally re-designated 833d Convalescent Camp with a 400-bed capacity.
On the continent, the 7th Convalescent Hospital with a capacity for handling 1,700 patients/trainees and the 8th Convalescent Hospital with a capacity for treating 2,000 convalescent patients, were operating under the Advance Section, Communications Zone.
Capacity for Convalescent Patients (31 Dec 44)
United Kingdom – 11,500 patients
Continent (France) – 4,000 patients
(at the end of 1944, convalescent patients/trainees in the 5 Convalescent Centers in the UK and the 2 Centers in France, numbered 13,600 –ed).
In December 1944, the Rehabilitation Division departed the United Kingdom for Paris, France. At the time, the Division consisted of the following Officers:
Colonel Rex L. Diveley – Chief, Rehabilitation Division
Major Julian A. Sterling – Assistant Chief, Rehabilitation Division
Colonel Milton S. Thompson – Rehabilitation, Liaison Officer to the G-3 Section, ETOUSA
Major Richard F. Kelsey – Consultant, Rehabilitation & Hospital and Convalescent Center Inspector
Major Blaise P. Salatich – Rehabilitation Liaison Officer, US Strategic Air Forces
Major Henry Heim – Coordinator, Information & Education Activities
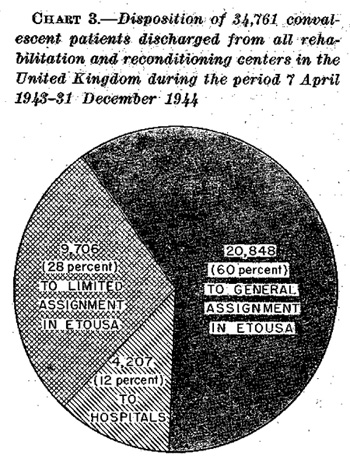
Chart illustrating the disposition of 34,761 convalescent patients from the Rehabilitation and Reconditioning Centers operating in the United Kingdom.
In the United Kingdom, Major William M. Brewer, MC, O-251177, was appointed Chief, Rehabilitation Division. He was assisted by 1st Lieutenant Andrew M. Gould Administrative Assistant (Major W. M. Brewer was transferred to the 750-bed 327th Station Hospital in France around August 1945 – which had closed for operations in the UK 23 February 1945, and set up in the Hôpital Américain at Etampes, APO 887, 18 July 1945 –ed).
Major William M. Brewer, Chief Rehabilitation Division, United Kingdom Base and fellow Officer, Dr. Lloyd Stockwell in front of the Officers Club & Mess, 49th Station Hospital, Diddington, England, which operated Hospital Plant # 4204 until 28 August 1945.
On 8 January 1945, the Rehabilitation Division, Office of the Chief Surgeon, moved from London to Paris. Due to the large number of battle casualties in the ETO, some of the rehabilitation activities had to be curtailed, yet, both the 7th and the 8th Convalescent Hospitals did efficient work. In the meantime additional rehabilitation personnel were being trained at the School conducted by the 826th Convalescent Center located in the United Kingdom Base. On 21 February 1945, a special conference of the Hospital Centers Commanders and the local Base Surgeons was held and plans for overall Convalescent Rehabilitation on the Continent outlined A tentative convalescent facility was to be established within each Hospital Center.
On 25 February 1945, Colonel Frank E. Stinchfield (formerly CO, 307th Station Hospital –ed) was appointed Supervisor of Convalescent Rehabilitation in the United Kingdom. In addition to his current duties, he retained command of the 826th Convalescent Center.
While researching suitable sites for setting up Convalescent Rehabilitation facilities in France and Belgium (6 Convalescent Centers were contemplated –ed), plans were made to move the 828th Convalescent Center and several selected Stations Hospitals from the UK to France. Since 1 April 1945, patients were transferred to the ZI when they required more than sixty (60) days of hospitalization, with the burden for convalescent programs placed on the individual hospital. During the latter part of April 1945 meetings took place with regard to the redeployment of Convalescent Centers and personnel to the Zone of Interior. Following V-E Day, immediate plans were made to transfer the 826th Convalescent Center to the ZI. The unit officially closed 18 May 1945.
Closing of Convalescent Centers at 2400 hours – 18 May 1945
825th Convalescent Center – Packington Park
826th Convalescent Center – Stoneleigh Park
827th Convalescent Center – Barton Stacey
833d Convalescent Camp – Bromsgrove
Between December 1944 and June 1945, the Rehabilitation Division had trained 138 extra Officers and 585 EM. The Convalescent Centers in the United Kingdom had discontinued operations and disposed all their patients by 6 June 1945. They were now re-organized as Staging Areas for movement to the ZI, with supplies and personnel being prepared to maintain a convalescent facility for the US Occupation Forces in Europe.
Our sincere thanks to John Brewer, son of Major William McKelvey Brewer, MC (O-251177) who generously provided us with additional data and a photo of his Father, who served with the Rehabilitation Division in the United Kingdom.